



RIRS MINI MICRO PCNL
PCNL

RIRS MINI MICRO PCNL
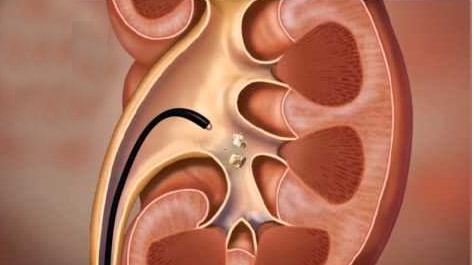
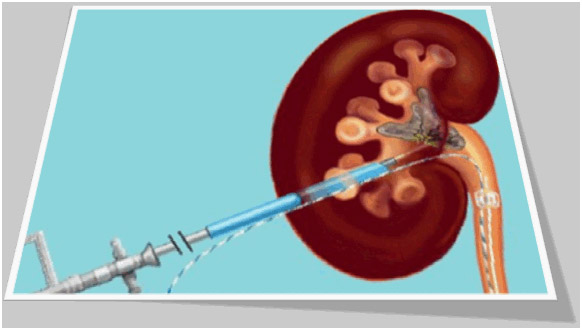
Retrograde Intra renal surgery for renal stone
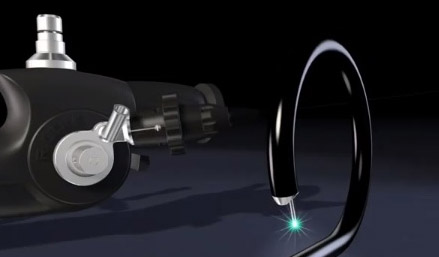
This is a Latest technology for the removal of kidney stone (size 8mm to 15mm). When lithotripsy fails to give result in kidney stone RIRS (Retrograde Intra Renal surgery) is the best method to treat kidney Stone. In this technology very thin flexible ureteroscope is passed from urethra through bladder and ureter into the kidney. Tip is deflected upto 270 degree so all the calyces of the kidney are visualized. Stone is located inside the calyx and with help of the holmium laser fibre stone is disintegrated into dust. Finally after total clearance of stone , D. J. stent is put to enhance the stone clearance.
What are the main advantages of this approach?
- Allows stone treatment without the need for any incision by using the urethra as the entry point
- Has a very high degree of success in treating stones
- Can be performed as day surgery
- More invasive compared with shock wave lithotripsy
- General anaesthetic required
- Small risk of damage to ureter (0.5%)
What are the main disadvantages?
- More invasive compared with shock wave lithotripsy - General anaesthetic required - Small risk of damage to ureter (0.5%)
Frequently Asked Questions (FAQs)
What are the advantages of RIRS compared to other stone treatments?
Provided that the kidney stones are an appropriate size and location, an advantage of flexible ureteroscopy is that it allows entry into all parts of the kidney. As long as the ureter is large enough to allow the ureteroscope to pass, there is a good chance that the stone can be broken and removed with one surgery.
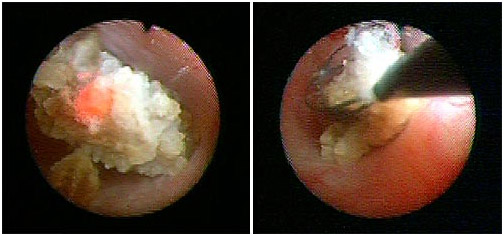
Compared to SWL, a kidney or ureteral stone can be seen under direct vision by the RIRS, allowing lithotripsy with lasers followed by basketting and removal. With shock wave lithotripsy, patients are asked to pass stone fragments themselves, causing potential additional pain or obstruction. Additionally, shock wave lithotripsy may not break up very dense, hard stones (termed SWL resistant stones). RIRS with a contact holmium laser can break up any stone, as long as the stone itself is accessible to the ureteroscope. Additionally, RIRS allows the treatment of stones are invisible on plain x-ray (acid stones).
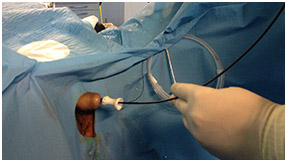
Compared to percutaneous procedures, the ureteroscope in RIRS is passed through natural body orifices and involve no skin incisions. It is an outpatient procedure, where PCNL requires at least an overnight hospital stay. Certain patient groups who cannot be treated with ESWL or PCNL (such as patients on blood thinners, women who are pregnant, the morbidly obese, and airline pilots/astronauts) can be treated safely and effectively by ureteroscopy.
Who is not a good candidate for RIRS?
Patients with large stones: Because RIRS requires active removal of all or most stone fragments, the treatment of very large stones (>2 cm) may yield so many fragments that complete removal becomes impractical or impossible. Patients with a history of urinary tract reconstruction: The anatomy of patients who have undergone ureteral or bladder reconstruction may not allow for passage of a ureteroscope. Patients who are intolerant of stents: As stents are usually almost routinely following ureteroscopy, patients with a history of stent intolerance may be more comfortable with other stone approaches.
What are the success rates of RIRS?
Depending on stone size, location, and number, success rates vary anywhere from 50% - 90%. Ask your surgeon to discuss success rates tailored to your particular stone disease.
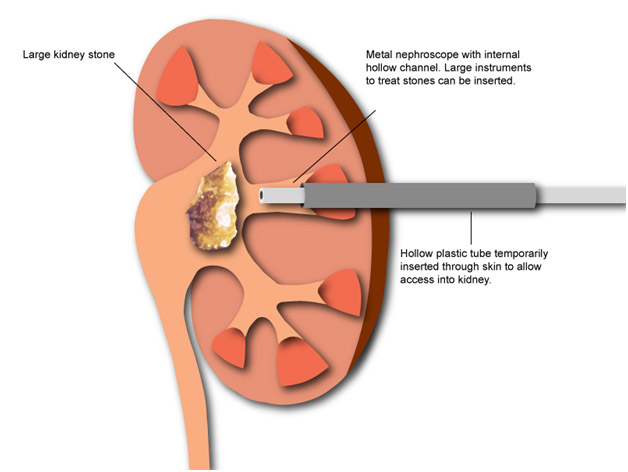
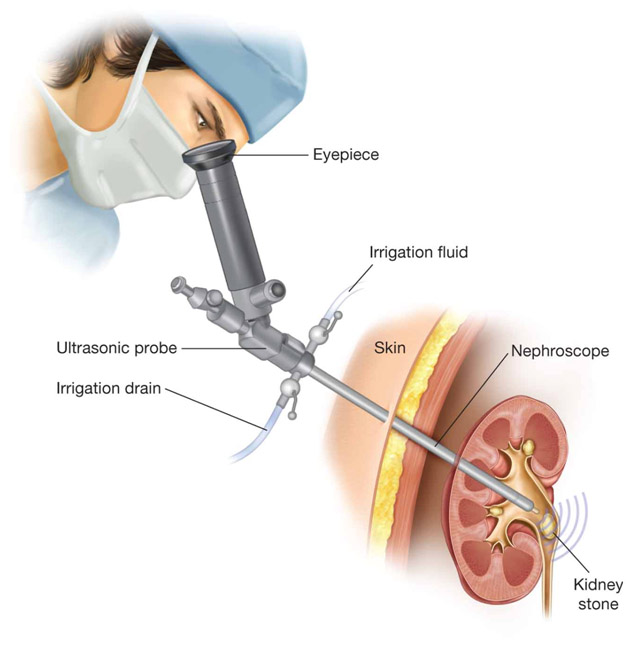
PCNL
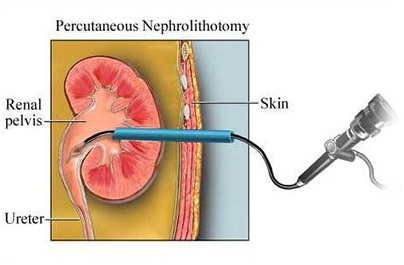
What is it?
Percutaneous NephroLithotomy (PCNL) is the preferred technique for treating larger kidney stones (over 2cm in diameter) located within the kidney. It involves keyhole surgery that is performed through a 1cm incision in the skin .
What are the advantages?
Allows for large or complicated stones to be treated in a minimally invasive fashion, which in the past this would have necessitated a large incision, and longer hospital stay. Hospital stay is now 2-4 days, and the out of hospital recovery time is significantly shorter than the traditional open surgical approaches. Quicker return to work. Compared to traditional techniques in dealing with large complex stones, there are no disadvantages. Improvements in techniques and equipment have allowed this type of surgery to be carried out more safely amongst subspecialty trained surgeons.
What are the disadvantages?
What are the risks?
This form of surgery is low risk if performed by a urologist who is specifically trained in this technique, and aided by meticulous pre-operative planning. The specific risks are uncommon but include infection, excessive bleeding (necessitating blood transfusion 5%, angio-embolisation 1%, or open renal exploration 0.5%), and adjacent organ injury (spleen, liver, bowel, lung, and diaphragm).
Frequently Asked Questions (FAQs)
What is the advantage of PCNL as compared to other stone treatments?
The primary advantage of PCNL over other treatments such as ESWL or ureteroscopy is that it provides a minimally invasive approach to treating and removing large stone burden in a single setting as compared to the need for multiple surgeries with the other therapies mentioned.
Are there disadvantages?
Whereas ESWL and ureteroscopy can be performed under intravenous sedation, PCNL requires a general anesthesia. Some patients may not be able to tolerate a general anesthesia due to their medical condition(s). As compared to other stone treatments, PCNL is slightly more invasive carrying with it a slightly higher risk. However, for most patients with large stone burdens, multiple stones or stones resistant to other forms of treatment, the benefits of PCNL outweigh the risks.
Which patients are good candidates for PCNL?
PCNL is an excellent option for patients with large kidney or ureteral stones (generally > 2 cm), multiple large stones, or stones resistant to prior treatment with ESWL or ureteroscopy.
What patients are not good candidates for PCNL?
Patients who have severe heart or lung conditions or have an uncorrectable bleeding propensity are not good candidates for PCNL. Patients with an active urinary infection are at a higher risk of sepsis during surgery and therefore should be treated with antibiotics to clear up the urinary infection prior to PCNL.
Can multiple stones be treated simultaneously with PCNL?
Multiple stones can be treated with PCNL. This is one of the advantages of this approach as a flexible telescope can be passed through the skin and directly into the kidney to attempt identification and removal of multiple stones in one setting. However, at times it may be difficult to visualize all areas of the collecting system despite the use of flexible telescopes and therefore some stones may not be retrievable. This may require placement of a second needle tract to access the remaining stones or a second PCNL procedure at a later date. Alternatively, PCNL can be used to remove the majority of the stone burden with ureteroscopy and ESWL left to clean up the remaining stone fragments.
Retrograde Intra renal surgery for renal stone
This is a Latest technology for the removal of kidney stone (size 8mm to 15mm). When lithotripsy fails to give result in kidney stone RIRS (Retrograde Intra Renal surgery) is the best method to treat kidney Stone. In this technology very thin flexible ureteroscope is passed from urethra through bladder and ureter into the kidney. Tip is deflected upto 270 degree so all the calyces of the kidney are visualized. Stone is located inside the calyx and with help of the holmium laser fibre stone is disintegrated into dust. Finally after total clearance of stone , D. J. stent is put to enhance the stone clearance.
What are the main advantages of this approach?
Allows stone treatment without the need for any incision by using the urethra as the entry point Has a very high degree of success in treating stones Can be performed as day surgery More invasive compared with shock wave lithotripsy General anaesthetic required Small risk of damage to ureter (0.5%)
What are the main disadvantages?
More invasive compared with shock wave lithotripsy General anaesthetic required Small risk of damage to ureter (0.5%)
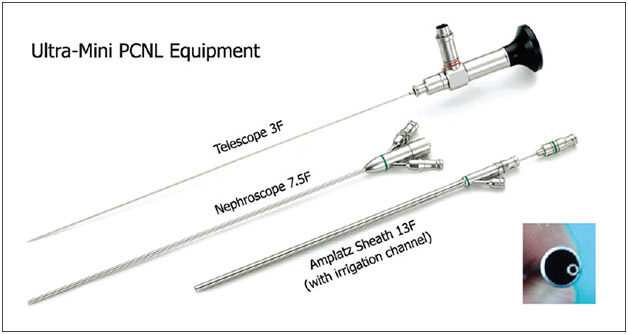
Mini PCNL , Micro PCNL and Ultra Micro PCNL
Mini Percutaneous Nephrolithotomy (Mini-PCNL)
The mini percutaneous nephrolithotomy is a new form of the procedure that follows the PCNL, except in its use of a smaller or miniaturized version of a nephroscope and Advanced Holmium Lasers . This approach to kidney stone treatments has been found to be nearly 100% effective when removing stones between 0.4 and 1 inch in diamete
Benefits of MINI PCNL over Traditional PCNL Procedures
Low-risk procedure. Small Puncture - Minimum blood loss. Reduce operative time. Minimum dilation of the tissue. Minimum Trauma. Lower operating time. 99% effective in removing stones of 1 to 2.5 cm in size. MINI PCNL used in Large Stone removal also. Fast Recovery. Minimum hospitalization.
Procedure of MINI PCNL
A special miniaturized Nephroscope used for Mini-PCNL. The surgery takes place under general anaesthesia. After contrast medium imaging of the kidney tract on the effected side, the kidney is punctured directly through the skin in the area of the flank. The puncture is controlled via fluoroscopy and ultrasound. A small hollow tube is placed directly through a patients back into the kidney through which instruments can then be used to fragment and extract the stone(s). Using a special laser, the kidney stones are then broken up and washed out. At the end of surgery, a catheter is placed in the kidney to secure the outward urine flow. This catheter can generally be removed without any pain a few days after surgery.