



Bladder Cancer
Bladder Cancer
Surgery is part of the treatment for most bladder cancers. The type of surgery done depends on the stage (extent) of the cancer.
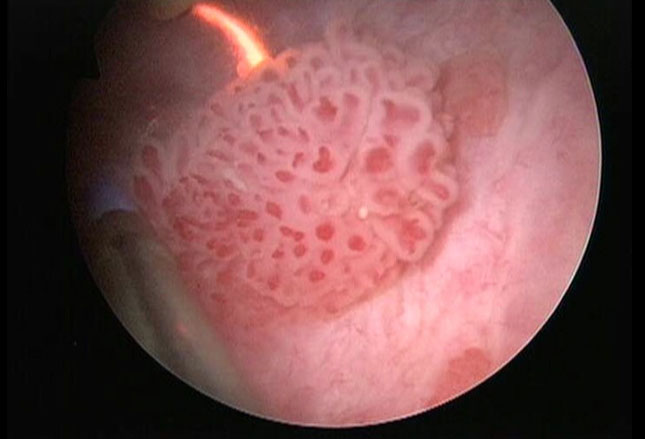
Transurethral resection of bladder tumor (TURBT)
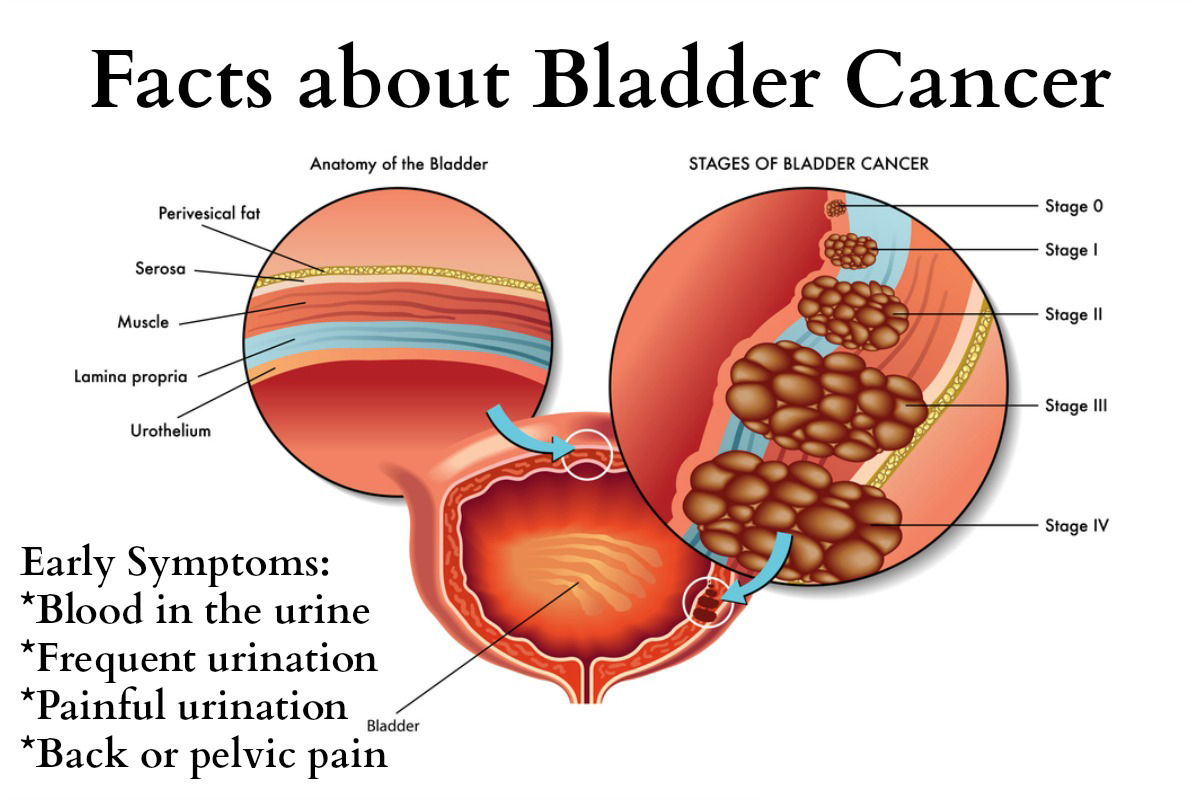
A transurethral resection of bladder tumor (TURBT), also known as just a transurethral resection (TUR), is often used to determine if someone has bladder cancer and, if so, whether the cancer has invaded the muscle layer of the bladder wall.
This is also the most common treatment for early-stage or superficial (non-muscle invasive) bladder cancers. Most patients have superficial cancer when they are first diagnosed, so this is usually their first treatment. Some people might also get a second, more extensive TURBT as part of their treatment.
How TURBT is done
This surgery is done using an instrument put up the urethra, so it doesnt require cutting into the abdomen. You will get either general anesthesia (where you are asleep) or regional anesthesia (where the lower part of your body is numbed).
What are the main disadvantages?
For this operation, a type of rigid cystoscope called a resectoscope is placed into the bladder through the urethra. The resectoscope has a wire loop at its end to remove any abnormal tissues or tumors. The removed tissue is sent to a lab to be looked at by a pathologist.
After the tumor is removed, more steps may be taken to try to ensure that it has been destroyed completely. Any remaining cancer may be treated by fulguration (burning the base of the tumor) while looking at it with the cystoscope. Cancer can also be destroyed using a high-energy laser through the cystoscope.
Cystectomy
When bladder cancer is invasive, all or part of the bladder may need to be removed. This operation is called a cystectomy.
Partial cystectomy: If the cancer has invaded the muscle layer of the bladder wall but is not very large and only in one place, it can sometimes be removed along with part of the bladder wall without taking out the whole bladder. The hole in the bladder wall is then closed. Nearby lymph nodes are also removed and examined for cancer spread. Only a small portion of people with cancer that has invaded the muscle can have this surgery.
The main advantage of this surgery is that the person keeps their bladder and doesnt need reconstructive surgery (see below). But the remaining bladder may not hold as much urine, which means they will have to urinate more often. The main concern with this type of surgery is that bladder cancer can still recur in another part of the bladder wall.
Radical cystectomy: If the cancer is larger or is in more than one part of the bladder, a radical cystectomy will be needed. This operation removes the entire bladder and nearby lymph nodes. In men, the prostate and seminal vesicles are also removed. In women, the ovaries, fallopian tubes (tubes that connect the ovaries and uterus), the uterus (womb), cervix, and a small portion of the vagina are often removed along with the bladder.
General anesthesia (where you are in a deep sleep) is used for either type of cystectomy.
Typically, these procedures are done through a cut (incision) in the abdomen. You will need to stay in the hospital for about a week after the surgery. You can usually go back to your normal activities after several weeks.
In some cases, the surgeon may operate through several smaller incisions using special long, thin instruments, one of which has a tiny video camera on the end to see inside the pelvis. This is known as laparoscopic, or keyhole surgery. The surgeon may either hold the instruments directly or may sit at a control panel in the operating room and maneuver robotic arms to do the surgery (sometimes known as a robotic cystectomy). This type of surgery may result in less pain and quicker recovery because of the smaller incisions. But it hasnt been around as long as the standard type of surgery, so its not yet clear if it is equally as effective.
It is important that any type of cystectomy be done by a surgeon with experience in treating bladder cancer. If the surgery is not done well, the cancer is more likely to come back.
Reconstructive surgery after radical cystectomy
If your whole bladder is removed, you will need another way to store urine and and remove it. Several types of reconstructive surgery can be done depending on your medical situation and personal preferences.
Incontinent diversion: One option may be to remove a short piece of your intestine and connect it to the ureters. This creates a passageway, known as an ileal conduit, for urine to pass from the kidneys to the outside of the body. Urine flows from the kidneys through the ureters into the ileal conduit. One end of the conduit is connected to the skin on the front of the abdomen by an opening called a stoma (also known as a urostomy).
After this procedure, a small bag is placed over the stoma to collect the urine, which comes out continuously in small amounts. The bag then needs to be emptied once it is full. This approach is sometimes called an incontinent diversion, because you no longer control the flow of urine out of the body.
Continent diversion: Another way for urine to drain is called a continent diversion. In this approach, a pouch is made from the piece of intestine that is attached to the ureters. One end of the pouch is connected to an opening (stoma) in the skin on the front of the abdomen. A valve is created in the pouch to allow urine to be stored there. You then empty the pouch several times a day by putting a drainage tube (catheter) into the stoma through the valve. Some people prefer this method because there is no bag on the outside.
Neobladder: A newer method routes the urine back into the urethra, restoring urination. To do this, the surgeon creates a neobladder basically a new bladder made of a piece of intestine. As with the incontinent and continent diversions, the ureters are connected to the neobladder. The difference is that the neobladder is also sewn to the urethra. This lets the patient urinate normally. Over several months, most people regain the ability to urinate normally during the day, although many people might still have some incontinence at night.
If the cancer has spread or cant be removed with surgery, a diversion may be made without removing the bladder. In this case, the purpose of the surgery is to prevent or relieve blockage of urine flow, rather than try to cure the cancer.